How Effective Are The Covid 19 Vaccines?
Executive Summary
- There has been a greatly oversimplified explanation of the effectiveness and safety of covid 19 vaccines.
- We cover some of the studies on this topic.
Introduction
Western health authorities and media have been nearly entirely focused on funding and promoting historically quickly-created coronavirus vaccines as the approved public policy response to the coronavirus. The pharmaceutical-controlled major media entities immediately hailed these vaccines as highly effective and safe.
Our References for This Article
To see our references for this article and related Brightwork articles, visit this link.
The Effect and Safety of the Vaccines
The following is a quotation from an excellent book on health policy and Covid 19 called Why Most of What You Know About Covid is Wrong.
Read the quotes, however, I will have an additional overlay that questions even this skeptical analysis of the studies that the FDA used to provide appoval for these vaccines.
Vaccine #1: The AstraZeneca Vaccine
So it is possible that the AstraZeneca vaccine causes traverse mylitas. In a small portion of those vaccinated at present, it seems like the risk of developing travers myelitis after getting the vaccine is about one to 3000. But it could be much higher or much lower. We don’t know until many more people have received the vaccine.
Would I take this vaccine personally No, because I’m young and healthy, and I therefore estimate that the risk of me getting severe COVID is infinitesimal. And I’m not convinced that the benefits outweigh the potential harms, considering the possible risk of transverse myelitis where I let my children to have it, no way not until there are studies showing that it’s safe and effective in children. It’s all it’s only a little over a decade since an influenza vaccine was rushed through and given to children based on limited evidence causing hundreds in Europe to develop narcolepsy, debilitating, lifelong disease.
Vaccine #2: The Pfizer Vaccine
With a Pfizer vaccine among those getting the placebo point 9% develop symptomatic COVID. And among those getting the vaccine point 0.5% develop symptomatic COVID.
That’s a 95% relative risk reduction and it is highly statistically significant. That is an impressive result much better than I ever would have thought would be possible in such a short space of time.
I use quotes and my analysis later to show that the above analysis is problematic. The issue is the relative risk reduction that is being quoted. I will illustrate how the statistical significance of this effectiveness is entirely irrelevant to the question of whether the Pfizer vaccine should have been approved.
The curious thing about this is that the author of the quote above, Dr. Sebastian Rushworth, is entirely aware of how pharmaceutical companies use relative risk to lie about the effectiveness of their drugs and that statistical significance is extensively used to mislead. This is explained very well in Dr. Rushworth’s following quotation.
Dr. Rushworth on the Misuse of Statistical Significance
I think the three main reasons are publication bias, vested interests that do what they can do to manipulate studies and the inappropriate use of the 5% p value cut off. That is why we should never put too much trust in a result that has not been replicated. We discussed statistical significance a lot now, but that isn’t really what matters to patients, what matters. And what patients care about is clinical significance, ie if they take a drug will it and have a meaningful impact for them.
Dr. Rushworth on the Misuse of Relative Risk
Clinical significance is closely tied to the concept of absolute risk and relative risk. Let’s say we have a drug that decreases your five year risk of having a heart attack from 2%. From point 2% 2.1%. Now the absolute risk reduction when you take this drug is 1% over five years.
Not very impressive, right? Would you think it was worth taking that drug? Probably not? What if I told you that the same drug actually decreased your risk of heart attack by 50%? Now you definitely want to take the drug right? How can a drug only decreased risk by point 1%, and yet at the same time, decrease risk by 50%. Because the risk reduction depends on if we’re looking at absolute risk or relative risk.
Although our imaginary drug only causes a point 1% reduction in absolute risk, it causes a 50% reduction in relative risk. drug companies will generally focus on the relative risk when discussing the benefits of their drugs, because it makes a benefit sound more impressive and absolute risk when discussing harms because it makes a harm sound small. When you look at an advertisement for a drug always look at the fine print, or they’re talking about absolute risk or relative risk.
However, Dr. Rushworth did not tie together his knowledge of the abuse of absolute risk in his analysis of the vaccine studies submitted to the FDA. At this point, let us continue with Dr. Rushworth’s analysis of the vaccine studies.
I will return to the issue of relative risk later in the article.
The result appears at first sight to hold up even for people aged 75 and older, with five cases among those getting placebo and zero cases among those getting the vaccine. Unfortunately, due to the small size of the group, the result is not statistically significant. So we can’t actually say based on this study, that the vaccine protects people aged 75 and older. With that said, the vaccine does seem to protect most people against infection.
Overall there were 240 events in the vaccine group that were classified as severe compared with 139 in the placebo group that is concerning several adverse events were 73% more common in the vaccine group than in the placebo group, the vaccine should ideally decrease severe adverse events. It shouldn’t increase them. Unfortunately Pfizer aren’t kind enough to provide a breakdown of what the adverse events are so it’s impossible for us to figure out whether the drastic increase in severe adverse events after vaccination is something we need to be concerned about and whether it should cause us to avoid the vaccine. Would I personally be willing to take the Pfizer vaccine. No, first of all because Pfizer hasn’t presented a detailed breakdown of what the adverse events are. So, what I can show that I can tell if there’s something in there that I should be worried about.
Rushworth catches the fact that Pfizer deliberately left out the severe adverse event detail, which did not stop the FDA from approving their vaccine, as the FDA is in the pocket of drug companies.
Vaccine #3: The Moderna Vaccine
As for the Moderna vaccine among those who had received the placebo injections 1.3% develop COVID, among those who had received the vaccine .07% develop COVID That represents a 94% reduction in cases 1% of the participants in the placebo group, experienced a serious adverse event and 1% of the participants in the vaccine group experienced a serious adverse event.
Overall the moderna vaccine does appear to be both effective and safe for two months of follow up, would I be willing to take it.
Yes, maybe two months of follow up is short so I would rather wait a few months more to see that the vaccine is truly safe, but I feel more convinced by what my journal has made public than I am by what AstraZeneca and Pfizer have put forth.
Dr. Rushworth Continues
All Three Vaccines
So let’s wrap up.
All three vaccines appear to be highly effective in preventing relatively young, healthy people from developing symptomatic COVID Although both the Pfizer vaccine and the modern a vaccine are clearly more effective than the AstraZeneca vaccine in terms of safety.
I have significant concerns about the AstraZeneca vaccine.
I also have concerns about the Pfizer vaccine.
Since there was a 73% increase in severe adverse events. Among those taking the vaccine. An issue that Pfizer hasn’t bothered to address at all and I’m also concerned about the fact that Pfizer does not provide a detailed breakdown of adverse events.
The Moderna vaccine does appear to be safe. However, Based on the data available up to now.
Finally, none of these studies can tell us whether the vaccines are safe and effective in children, it would be unethical to start vaccinating children without first having made sure that the vaccines are safe for them. Especially considering that the risk to children from COVID is infinitesimal. – Why Most of What You Know About Covid is Wrong
How the Covid Vaccine Studies Were Rigged
The drug companies have rigged the studies to make the vaccines appear more effective than they are.
- The drug companies had a massive financial bias in doing these studies, and as with all FDA-reported studies, they only reported the studies they wanted to and would have been able to hide those that were less impressive.
- The drug companies selected the duration of the studies they wanted and never had any oversight from the FDA on study length.
- They minimized the trial length so that adverse reactions would be minimized.
- The FDA was under extreme pressure from the Trump Administration to approve the vaccines, and the interference and pressure brought by the Trump Administration are well documented.
- The drug companies misleadingly chose primarily young and healthy test subjects.
- They also hid and downplayed the negative consequences of taking the vaccine.
- Neither the drug companies nor the FDA addressed that the protection offered by the vaccines, unlike previously developed vaccines, declines over time, necessitating the need for “booster shots,” which are later vaccine doses to increase antibodies once again.
Because these drug companies are compelling and the FDA’s standards were lowered due to Trump’s Operation Warp Speed, they could get these highly profitable vaccines approved by the FDA with one study each.
Many other treatments have far more studies and far better evidence for their effectiveness. Still, because they are not the preferred treatment of drug companies, they are not considered competing treatments.

This listing of other treatments against Covid 19 that show similar effectiveness, many of which can be taken before contracting Covid. Many of these drugs do not have many studies performed on them.
- Why have governments not been sponsoring more studies in this area if this is such an important issue?
- Why are US health authorities and establishment media entirely disregarding these treatments?
This second topic is explained in the following quotation from the website.
Pharmaceutical drug trials often have conflicts of interest whereby sponsors or trial staff have a financial interest in the outcome being positive. Ivermectin for COVID-19 lacks this because it is off-patent, has many manufacturers, and is very low cost. In contrast, most COVID-19 ivermectin trials have been run by physicians on the front lines with the primary interest of finding the best methods to save human lives and minimize the collateral damage caused by COVID-19. While pharmaceutical companies are careful to run trials under optimal conditions (for example, restricting patients to those most likely to benefit, only including patients that can be treated soon after onset when necessary, ensuring accurate dosing), many ivermectin trials do not represent the optimal conditions for efficacy.
And next, the website explains the pharmaceutical company’s incentive to produce studies that undermine off-patent drugs.
Two ivermectin trials to date involve very large financial conflicts of interest [López-Medina, Together Trial] — companies closely involved with the trial or organizers stand to lose billions of dollars if ivermectin efficacy becomes more widely known. The design of these trials favors producing a null outcome as detailed in [López-Medina, Together Trial]. Note that biasing an RCT to produce a false positive result is difficult (suppressing adverse events is relatively easy [Evans]), but biasing a trial to produce a false negative result is very easy — for example, in a trial of an antiviral that works within the first 24 hours of symptom onset, trial organizers only need to avoid treating people within the first 24 hours; or with a disease like COVID-19, organizers only need to select a low-risk population where most people recover quickly without treatment.
We note that, even under the very suboptimal designs, these trials produced positive results, although without statistical significance.
How Establishment Media Entities Act as Public Relations for Pharmaceutical Companies
Anyone who proposes using any of these treatments is immediately attacked and discredited as anti-science by the establishment media. Most of these studies are less biased and more scientific than those that cause the FDA to approve the vaccines. Why are these studies not considered science, while the FDA’s approved Big Pharma rigged studies are considered science? Is science simply whatever the large pharmaceutical companies say it is?
This is a very standard piece of coverage by the establishment media. Children have essentially zero risk from Covid 19, and none of this is brought up in the segment. There is no opposing viewpoint and no explanation or analysis of the vaccine.
The article How Pharma and Media Lied About Covid Risks to Children for Maximum Profits covers much more on how the media and pharmaceutical companies lied on this topic.
Most Common Symptoms of Covid
The most common symptoms in people with long COVID defined in the study is still having symptoms after four weeks or fatigue, 98% and intermittent headaches 91% these are both extremely nonspecific symptoms, there is nothing about them that is specific for COVID.
In fact, there are some of the most commonly reported symptoms of post viral syndrome, suggesting that long COVID and post viral syndrome are to a large part, one in the same. First, long COVID is rare, around one in 50 people still have symptoms at the 12 week mark and since a number with symptoms drops significantly, at one two and three months it is likely that the reduction continues after 12 weeks and that is a tiny fraction that still has symptoms at six months. – Why Most of What You Know About Covid is Wrong
Long covid is critical in scaring the population into scaring parents into vaccinating children.
These videos prove that the media assiduously reported precisely what the pharmaceutical companies wanted them to say.
Update as of October 2021
What Has Been the Effectiveness of the Vaccines in the Field?
The effectiveness of treatments, mainly when performed by a biased entity, is nearly always lower in the field than during clinical trials.
The FDA and the establishment media are quick to report on the effectiveness of treatments but are silent on the efficacy of treatment in the field.
This is explained in the following quotation.
Even though the unvaccinated are coerced to test more frequently for travel, education and work, their numbers are still similar to the “fully vaccinated.” The data shows that COVID cases are relatively equal among the vaccinated and unvaccinated. From August 21, to September 17, 2021, there were 69,639 positive cases recorded among the unvaccinated population, and 79,613 cases among the vaccinated population, with 60,923 of these cases deriving from the “fully vaccinated.” Clearly, the vaccine doesn’t prevent COVID, and may even be a driving force for new infections in the unvaccinated.
Most shocking, the rate of death is not 95 percent lower in the vaccinated group. From August 14 to September 10, 2021, Scotland registered 208 covid-19 deaths. There were 41 deaths in the unvaccinated, 9 deaths in the partially vaccinated, and a shocking 158 deaths in the fully vaccinated. If the 95 percent efficacy of the vaccine was real, then 95 percent of the deaths would occur in the unvaccinated and only 5 percent would be in the vaccinated. However, up to 80 percent of the deaths are in the vaccinated and only 20 percent of the deaths are in the unvaccinated. The vaccines are currently INCREASING the risk of death in the UK by 400%! – NewsTarget
Were the Vaccines Scientific Fraud? Relative Versus Absolute Risk
“That 95% refers to the ‘relative risk reduction’ (RRR), but it doesn’t tell you how much your overall risk is reduced by vaccination. For that, we need ‘absolute risk reduction’ (ARR).
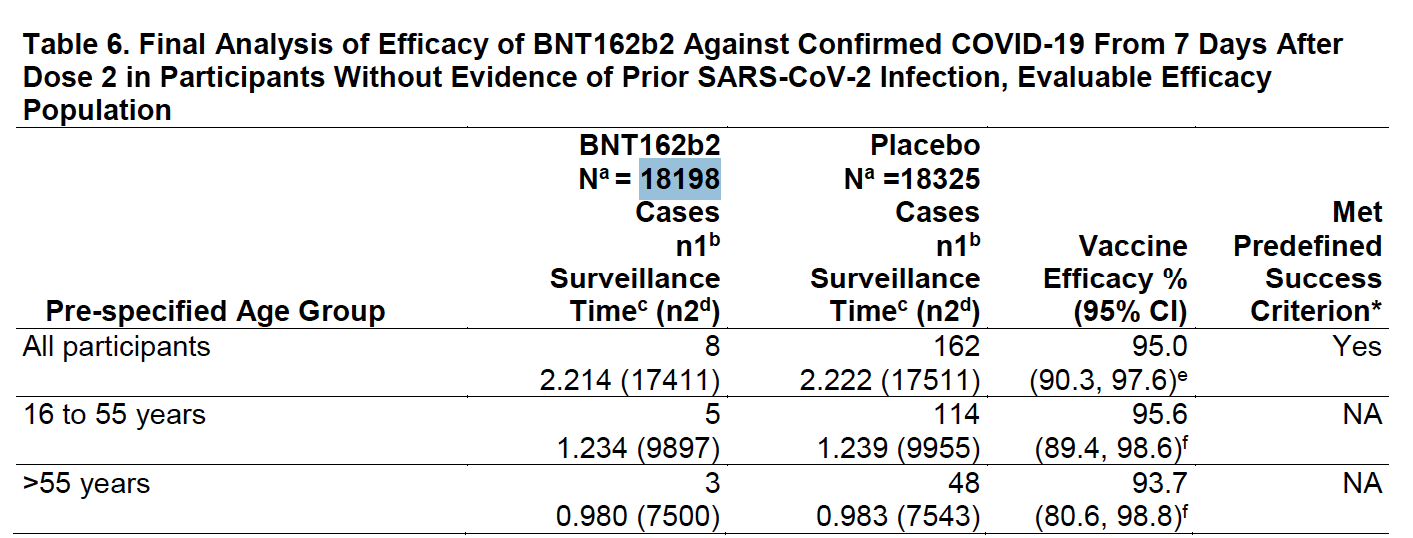
“In the Pfizer trial, 8 out of 18,198 people who were given the vaccine developed COVID-19. In the unvaccinated placebo group, 162 people out of 18,325 got it, which means that even without the vaccine, the risk of contracting COVID-19 was extremely low, at 0.88%, which the vaccine then reduced to 0.04%.
Let us lay out the math on this so it is more clear.
- 8 (those given the vaccine that developed covid) / 18198 (the total number given the vaccine) = .0004
- 162 (those not given the vaccine that developed covid) / 18325 (the total number given the vaccine) = .0088
- .0088 (unvaccinated who got the virus) – .0004 (vaccinated who got the virus) = .0084 or .84%. This must be multiplied by 119 times to equal 1%.
However, to obtain the relative risk (that is what Pfizer, the FDA, and establishment media reported), it is given by 1 – (8/162) or 95%.
That is entirely misleading. This math is available on the FDAs EUA approval of the Pfizer vaccine, and these are simply Pfizer’s numbers.
That is the Pfizer vaccine.
Let us see the table I have taken from the Moderna FDA EUA (or Emergency Use Authorization).
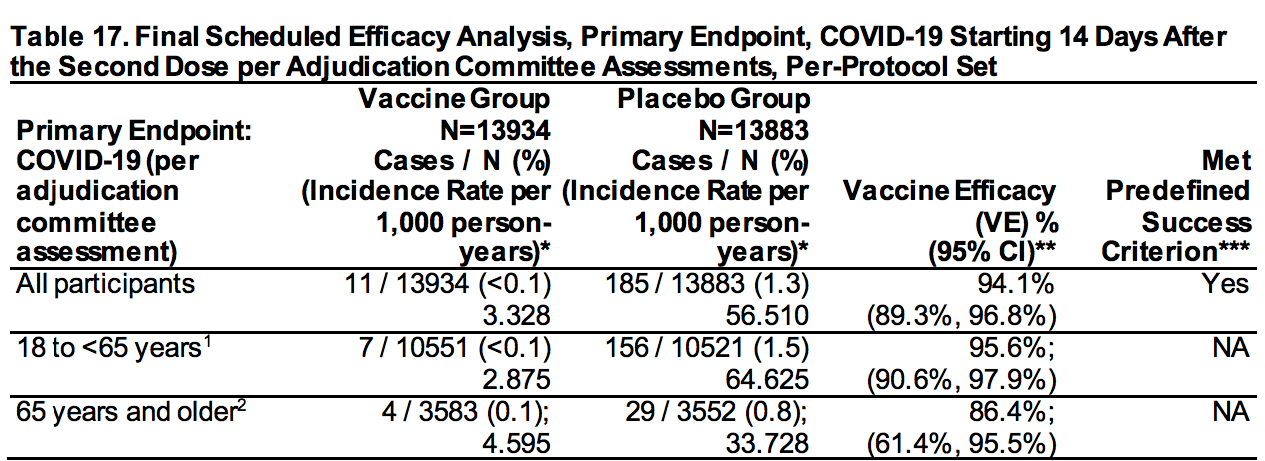
I will just be focusing on the entire line at the top.
- 11 (those given the vaccine that developed covid) / 13934 (the total number given the vaccine) = .0006
- 185 (those not given the vaccine that developed covid) / 13883 (the total number given the vaccine) = .0138
- .0138 (unvaccinated who got the virus) – .0006 (vaccinated who got the virus) = .0132 or 1.32%.
However, one takes 1 – (11/185) using relative risk to obtain 94%.
More Clinical Trial Math Analysis
This math is analyzed in the following quote from the article What Can Statins Teach Us About The COVID-19 Vaccines?
When the initial Pfizer vaccine study was published in the Lancet, all of my colleagues were captivated by the claim the vaccine was “95% effective,” and they all repeated the mantra, “well, we had hoped the vaccine would work, but we never imagined it would be this effective.” I took a look at Pfizer’s study and noticed that:
You had to vaccinate 119 people to prevent one minor case of COVID-19 (e.g., a sore throat + a positive test), 2711 people to prevent one “severe” case of COVID-19 (“severe” never being defined), and since no deaths were prevented in the trial, well over 21,720 people needed to be vaccinated (21,720 is the total number who were vaccinated in the trial) to prevent a single death from COVID-19. Additionally, the vaccine’s ability to prevent transmission was never assessed, and based on my knowledge of the vaccine design (which was unlikely to prevent transmission), it was unlikely to do so.
However, even this math was later proven to overstate the effectiveness of the vaccines as the studies were so shoddily performed and so rigged (points which I will address further in this article) that none of the data points from the study are reliable. The terrible math of the vaccines is reinforced in the following quotation.
Addressing the Damage
One of the best ways to address the damage caused by the covid vaccines is with Ivermectin. This is the reason I began taking Ivermectin -- before investigating all the other health benefits of the drug. Now, I take Ivermectin for many reasons.
- We have Ivermectin dosage calculators based on research studies and for all the different uses of Ivermectin.
- We are the only web source offering an Ivermectin dosage calculator in addition to different dosage estimates for different cancer types.
- All of our calculators are easy to use (see our dosage calculator listing). Each person enters their personalized information into the calculator and receives our recommended extensively researched dosage estimate automatically and immediately calculated.
- We also cover the broader problems with dosage calculation in medicine at the article The Problem With Dosage Calculation in Medicine, as this is an issue much larger than for one drug.
About Our Ivermecting Testing Program and Recommended Ivermectin Source of Supply
- We performed pharmaceutical testing on Ivermectin to find a lower-cost version that also matched Merck's original Ivermectin in bioequivalence.
- You can read about the details of our Ivermectin testing in this article, Our Ivermectin Bioequivalence Testing.
- We got Summit Products to carry this version of Ivermectin, which passed our bioequivalence testing.