The Problem with Nigerian Doctors Practicing in First World Countries
Executive Summary
- Nigerian doctors have left their country in droves, and they have left for developed, primarily European based countries, leaving Nigerians without sufficient doctors. According to Western progressives, this is a “good thing.”
- The Nigerian culture of scamming seems to be following these doctors to their professions in their new countries.
Introduction
Professionals from third world countries who have migrated to first world countries have caused massive problems in several areas, including Indians working in IT, as we cover in the article How Indian IT Workers Discriminate Against Non-Indian Workers. In this article, we will cover the issues with Nigeran doctors.
Our References for This Article
If you want to see our references for this article and related Brightwork articles, see this link.
Why Nigerians Leave Nigeria
The article Doctor Drain in Ozy Magazine explains some of these reasons in the following quotation.
The hospital waiting room overflows with people. It’s an unusually hot day in Lagos, Nigeria, the temperature over 90 degrees Fahrenheit. Sweaty patients silently clasp their hands in prayer, hoping to see a doctor. In a nearby room, physicians wrestle with cords and switches on brand-new anesthetic and radiology machines from the U.K. that short-circuited during recurring power outages.
Africa’s largest economy is rapidly bleeding doctors it has trained and educated, unable — or unwilling — to stanch the flow that medical professionals blame on low salaries and poor working conditions. Approximately 20,000 Nigerian medical doctors are currently working outside the country. A survey by NOIPolls found that about eight out of 10 doctors who remained in Nigeria were looking for jobs overseas, with the U.S. and U.K. as leading destinations.
A crumbling medical infrastructure is pushing better-off Nigerians to seek treatment abroad. Last year, the Healthcare Federation of Nigeria reported an annual loss of $1 billion to the nation due to medical tourism. For those who can’t afford foreign treatment, it’s worse. The country currently has a doctor to patient ratio of 1 to 4,000, far higher than the World Health Organization’s recommendation of 1 to 600.
“Doctors [in Nigeria] are not well taken care of,” Elenwoke says. “We’re not a priority of the politicians.”
The presentation of this issue is a bit odd. Nigerian doctors are using the Nigerian health system’s work environment as an excuse to flee the country. As if Nigerian doctors deserve so much better than Nigerian standards!
This is because the limitations described above in medical facilities in Nigeria are the same issues throughout Nigeria. Why is this a surprise to Nigerian doctors? Are they not familiar with their own country?
The article describes the doctors as if they are almost apart from the Nigerian system — and that they are deserving of more modern facilities that are invariably in white countries, where not only the Nigerian doctors prefer to practice but also where they would choose to live. However, while Nigerian doctors can leave the country, many people have reached out to comment on why they should leave Nigeria as Nigeria is “below” these now-educated doctors.
Guess who can’t leave Nigeria?
That is right, Nigerian patients. Under this great empathy, which is directed to Nigerian doctors, which is supposedly quite progressive, what is not accounted for is what happens to Nigerian patients that are vastly underserved in heath — and a primary reason is that so many Nigerian doctors leave the country so they can work in conditions in white countries, that Nigeria 60 years after independence, the country still cannot figure out elementary sanitation procedures. So, the progressive and politically correct view leaves Nigeria significantly underserved by physicians because they go. The advanced view supports this because it means Nigerian doctors find a better life (always in white countries for some reason), while patients in Nigeria are left behind. This article explains what happens to the population when most doctors decide they deserve better than their home country.
Despite the critical need for doctors, Uganda’s government recently approved a plan to recruit over 200 doctors and nurses to Trinidad and Tobago. The Ugandan government promoted the initiative, maintaining that it could “further accelerate the existing excellent bilateral relations.” The Caribbean country has provided financial aid and training for Uganda’s oil and gas industry and its police force.
..a local think tank, the Institute of Public Policy Research Uganda (IPPR-U), challenged the wisdom of the government’s move. “While the government is bent on exporting health workers, thousands of Ugandans are dying daily,” the group said. “Sixteen women die daily giving birth.” The think tank took the matter to court, accusing the government of violating “the constitutional rights of Ugandans to access basic medical services.”
The entirety of the view is about the improvement in the life of Nigerian doctors receive and nothing about Nigerian patients. Thank you progressive and enlightened commentators! And of course, the most ardent supporters of this view are the Nigerian doctors themselves who can’t wait to create some type of rationalization for why they absolutely can no longer tolerate living in Nigeria. – UN.org
However, for progressive voices, the doctors, not the leftover patients, that matter. And it is considered racist not to allow Nigerian doctors to immigrate away from where there is a need (but is below them to serve Nigerian patients), to where there is a surplus, and to degrade the health systems in the first world countries with their third world nation corruption.
The following is also from UN.org, but on a slightly different dimension of the migration.
Africa’s loss is rich countries’ gain: the research estimated that financial benefits amounted to $2.7 billion to the UK, $846 million to the United States, $621 million to Australia and $384 million to Canada. Rich countries should provide financial and logistical support to Africa’s health institutions, the researchers recommended.
I would question these numbers.
First, why would first-world countries have a problem developing medical talent? Second, does this estimate include the corruption that Nigerian doctors bring to white countries? And what is the cost to the integrity of the overall healthcare system? Indeed, wages go down anytime outside labor supply is added, and physicians in the US are mostly overpaid.
The article in OZY Magazine presents this view as if it is somehow unique when virtually the entirety of Nigeria’s population would like to live in a white country. Remember, all countries and all cultures are equal, and any commentary to the contrary is just racism. Nigerians are routinely stopped and asked to pay bribes to police, so no, Nigeria is not considered a desirable place to live. Nothing in Nigeria works very well. But notice that each doctor seems to think they have no part in this dysfunctionality. And white progressives agree with them, of course. As I just stated, most of the people in Nigeria would like to emigrate to white countries because they are tired of the dysfunctionality of living in black-run societies. Blacks living in black cities are equally tired of living in these cities and leave at the first opportunity to try to find the highest concentration of white people that they can. But none of them bear any responsibility for the dysfunctionality of these areas. Isn’t that curious.
How is that possible?
And let us get this part out of the way.
Many Africans are taught that colonialists robbed them, which is why their respective country’s problems. The elite likes to present this story because it absolves them of any responsibility to provide things to their populations. Robert Mugabe was one of the biggest supporters of this storyline. However, Rober Mugabe also wrecked Zimbabwe’s economy, and his wife and sons specialized in shopping at high-end stores in Europe and robbing the Zimbabwe treasury. These are not things that the “evil white colonialists” compelled them to do. White colonialists have a habit of apparently visiting African kleptocrats and telling them to rob their constituents and then go shopping in the highest-end stores in Europe. These kleptocrats are renowned for their long lines of baggage carts of luxury goods found at the Charles de Gaul Airport, being taken back to Africa. This apparently has nothing to do with the African kleptocrats themselves and any decisions they make but due to the “legacy of colonialism.”
The white man is remotely controlling Mugabe’s children into pouring Crystal over their Rolexes. When will colonial powers stop doing this to the children of kleptocrats?
There is continual theft in the mining industry, covered in the article The Economist Misleads Again on Tanzania Versus Acacia Mining. However, in each case, the African government officials are paid off and complicit in tax evasion and labor mistreatment by (typically European) firms.
Colonialism or colonialist interactions also brought much technology to African countries. For example, no African today would have access to a train or cell phone if it were not for interactions with non-African countries. Before the European powers arrived for their brief stay, Africa had not developed the wheel. They did not have any broad usage of metallurgy. Any metal in sub-Saharan Africa came from North East Africa — close to Egypt. Small quantities of metal migrated from cultures outside of Sub-Saharan Africa, but none was made within Sub-Saharan Africa. Many even educated Africans have no idea about this and, of course, don’t want to know about it. Observe the following quote from a commenter.
What about countries like China or Japan or other countries who weren’t colonized, this things came there eventually didn’t they?
This commenter has no idea that, for example, all of the technology the Japanese used against other countries in WW2 was from Europeans. All one has to do to find this out is look up the Menji Restoration. China’s entire current manufacturing is based upon copying European/American/white technologies and stealing as much of the IP of European/American/white civilizations as it possibly can. However, in the current brainless climate, it is considered to have significantly evolved to a state that African countries have been hotbeds of innovation. Any observations about the natural history of innovation are hand-waved away with accusations of racism.
The lack of development of African countries cannot be perpetually laid at European colonial powers’ feet. African elites want this to be thought proper by their constituents, but it is not historically correct, and it prevents these countries from ever taking responsibility for their management. We cover in the article Why Do Most Europe Influenced African Countries Have the Least Slavery.
The European powers are not telling Africans to have too many children for African infrastructure or stopping them from printing enough books for schools (many African students have to share books as there are often not enough to go around.) The European powers are not stopping the Congo from having the mineral wealth of that Saudi Arabia has in oil and 1/2 of the country living on less than a dollar a day. That is the African elite that wants this state of affairs. They want to blame previously colonialist European countries for making them highly corrupt and stealing from the public treasury. The hand of the white man continues to make African leaders steal and take shopping trips to Paris. How this is happening is a mystery.
Equatorial Guinea’s oil reserves were found AFTER the country obtained independence. The elites are fabulously wealthy — these elites would not have this wealth if not for their relationship with other countries. That is, no African country could extract oil from their countries without help from outside.
However, the elites in Equatorial Guinea have ensured that almost none of the population has benefited from this oil — all with Africans being in control of the country, all after colonialism passed.
Nigerian Doctors Find Nigeria (a Black Run Country) Unacceptable and Prefer to Relocate to White Run Countries?
Like Elenwoke, Makanjuola has dreams for his country. He hopes to one day open a small medical school in Lagos and instruct doctors to practice medicine like they do in the U.S. and U.K. But it’s unlikely to happen. “Nigeria doesn’t want me back,” Makanjuola says. “There’s not enough pay, the security isn’t as good [as in the U.S.] and there are no policies in place to help.” Makanjuola believes the Nigerian government could afford to put more funds toward the medical sector if it wanted to, but it doesn’t seem to value human life enough. – Ozy
Makanjuola is Nigerian. Yet he believes he deserves medicine as it is practiced in the US and the UK. He thinks that Nigeria, a nearly 100% African country, will run medicine like a predominantly white country. Why would that be considered a reasonable expectation? And notice that if Nigeria cannot provide him with the standard of living and the medical standards of a white country, then Nigeria.
“..Does not want him back.”
Notice the following quotation, which again points out the unacceptable earnings of doctors in Nigeria.
“It has become worse; a doctor [in Nigeria] earns N200,000 monthly ($560), necessitating moving to countries where they can be better paid for their services … This ultimately means that eight of 10 Nigerians are presently receiving substandard or no medical care at all.” – Al Jazeera
Were any of these Nigerian doctors aware of what doctors in Nigeria were paid before they went through medical school, or was it a complete shock to them? Because it makes it sound like none of these doctors realized what Nigerian doctors were paid until after graduation.
Dysfunctionality Writ Large
Invariably, once groups can move from a low trusted third-world nation to a white or European-based country, these same groups bring their dysfunctionality with them. Nigerians, even among Africans, have a well-earned reputation as scammers. They are probably the country most associated with scamming anyone they come across. Part of the Nigerian culture is to esteem crafty people who can “pull one over” on other people. The international phone scams from Nigeria are well known, yet the government does little to crack down on them.
So, how does the scamming Nigeria culture fit with medical science?
The recent case of Bennet Omalu, the Nigerian doctor who appears to have misled people regarding the brain disease of CTE, is illustrative.
The Nigerian Doctor, Bennet Omalu
Here are some quotes from The Washington Post.
CTE experts, in interviews, did not dispute football damaged Webster’s brain. He probably played through many concussions, and the NFL’s retirement board acknowledged Webster suffered from football-related brain damage in 1999.
In medical research papers, it is customary to publish, as photos, the most compelling, striking images that depict the paper’s subject. The images Omalu published in the Webster paper do not show CTE, nor do they show alarming amounts of tau for a 50-year-old man, experts said.
The images show tau in formations called tangles. One image shows a single tangle, highly magnified, and another shows a similarly magnified image of two tangles, according to the paper. Both images come from the cortex.
McKee and other experts said one or two tangles can be found in the cortexes of otherwise healthy 50-year-olds. If surrounded by several other tangles, they could be part of a disease. But in isolation, they could be benign. It was as if Omalu had claimed to have found a rare species of bird and then, as proof, published a paper that included only a few close-up images of the tip of the beak.
In interviews, two of Omalu’s co-authors had conflicting memories about what they saw in Webster’s brain.
DeKosky, the Florida neurology professor, said he recalls seeing the signature CTE pattern but was unsure why the correct images weren’t selected for the paper.
The reason Omalu picked the wrong images, Davies said, was that Omalu “was not any kind of an expert.”
Omalu became internationally known for his claims about CTE. However, he is not able to support his initial claims. He is also being called out for being so inept in understanding his subject matter. He does not know what to look for in the images, and because of this, he took images of a healthy brain and included them as evidence of CTE.
The European-based research system has a foundation that the researchers will not merely make things up. However, Omalu is not from a European-based system but from Nigeria. European-based countries that allow migration from third-world countries like Nigeria, which have no concept of objectivity, are significantly in error if they think that just because doctors can graduate from medical school, they will follow European-based countries’ culture.
Omalu Misrepresenting the Studies of Others
No studies have found that merely playing a contact sport increases the risk of the tragic life outcomes Omalu has described. In some settings, when citing these figures, he has mentioned “a paper that came out of Sweden.” This appears to be a reference to research led by Seena Fazel, professor of forensic psychiatry at the University of Oxford, examining what happened to more than 1.1 million people in Sweden who suffered brain injuries before turning 25.
Fazel was unaware of how Omalu had been interpreting his studies until contacted by a reporter last year.
“That’s definitely not what we said. . . . You can’t extrapolate that from our work,” Fazel said in a phone interview.
This is another violation of the “rules of the road” for research. One does not appropriate the world of someone else, which is not applicable (serious brain injuries versus sports injuries). Secondly, why would Omalu not contact the research’s originators before submitting such statements to a court as an expert witness? This type of behavior and further quotations illustrate that Omalu should never be performing any research.
Omalu, Living the High Life in the US
Now 51, Omalu lives in Sacramento with his wife and two children. He works part-time as an associate professor at the University of California Davis, but the bulk of his income comes from work as an expert witness, he testified in a deposition last year. He charges a minimum of $10,000 per case and earned about $900,000 in 2018, he testified.
Judges have, on occasion, taken issue with Omalu’s reasoning. In 2016, a Pennsylvania judge, citing “numerous methodological errors,” dismissed Omalu as the only expert witness for an auto mechanic suing several chemical companies, alleging he had contracted Parkinson’s disease from welding solvents and fumes.
“Dr. Omalu admitted to knowing little to nothing about welding, the fumes generated, and publications concerning the topic. . . . [He] repeatedly testified that this subject is outside of his area of expertise,” wrote Judge Richard E. McCormick Jr., who also noted that Omalu never examined the man, didn’t read his testimony and had no information concerning the man’s working conditions and levels of exposure to various fumes. The case was dismissed.
In February 2018, Omalu filed a declaration in a federal lawsuit against the Pop Warner youth football organization in which he suggested playing football increased the risk of drug abuse, mental illness and death before 42, among a long list of harrowing life outcomes. The case was dismissed last month, with a ruling in which U.S. District Judge Philip S. Gutierrez wrote he found Omalu’s testimony “unreliable.”
In March, Omalu served in a role that doesn’t fit neatly into his self-promoted biography of the heroic doctor fighting corporate interests: He worked as an expert witness for Ford Motor Company, which was being sued on behalf of a 53-year-old man killed after being struck by an 8,700-pound metal device in one of the company’s assembly plants.
The local medical examiner had determined the man had lived — and probably suffered tremendous pain — for about 30 minutes after the accident. Omalu testified that he believed the man was killed instantly, and because the man had been a smoker, he had a reduced life expectancy, arguments that could reduce Ford’s financial liability.
Over the course of the two-hour deposition, Omalu claimed 100 percent of NFL players have CTE and suggested parents who let their children play football or soccer are committing child abuse.
At one point, a lawyer asked Omalu about the Pennsylvania case in which the judge dismissed him as an expert. That had nothing to do with his scientific expertise, Omalu insisted. It was because the judge was from Pittsburgh, he explained, and probably an NFL fan.
“Remember,” Omalu told the lawyer, “I discovered CTE.”
This is the behavior of a Nigerian scammer who has been allowed to persist in a scam as an immigrant because of the US’s accepting nature. Omalu is being called out by judges, who should never be in the position of calling out an expert witness. Why Omalu thinks he can get away with testifying on topics where he has no background fits in the pattern of fake expertise, as he did with CTE.
It also brings up the question of who is being called as an expert witness. This problem is severe as one can find an expert witness to support virtually any view, and the compensation is so high that it creates a great incentive to alter one’s beliefs to match whoever is paying the most.
Columbia Pictures, Sony Pictures, LStar Capital, Village Roadshow Pictures, Scott Free Productions, and all the companies producing Concussion should have researched Omalu’s medical research. If they had, they would have found that the story told by Omalu does not add up. Omalu has lost respect in the medical research community. He has ceased performing research for what we think is an excellent reason. If he were to publish more material on this topic, he would most likely become more exposed than he already has been.
The movie Concussion further distorted the CTE issue’s reality — beyond misrepresenting his research by creating concocted events to heighten the “drama,” as the following quotation describes.
But Landesman’s loosey-goosey docudrama standards are exactly the problem. When Omalu’s character says, at one point in the film, that “God did not intend for us to play football” and later warns that as long as we do, “men will continue to die,” he’s appealing not to fact-based objective truth but to an alternate reality—an emotional, spiritual one—that has come to dominate the enlightened person’s understanding of the NFL.
Are we actually watching players kill themselves before our eyes? No, not on average: A 2012 study of several thousand NFL retirees, conducted by researchers at the National Institute for Occupational Safety and Health, found that the former football players lived significantly longer than race- and age-matched controls. They were much less likely to die from cancer, heart disease, diabetes, accidental falls, or homicides than anybody else. That doesn’t mean that taking hits improved their health, of course; surely the opposite is true. But still this study gave the lie to a fundamental intuition about football and one that’s touted almost everywhere. There’s zero evidence that playing professional football shortens lives on average.
And in Concussion, his character makes the link explicit: In explaining the death of another former Pittsburgh Steeler, Terry Long, Omalu says, “Football gave him CTE, and CTE told his brain to drink a gallon of antifreeze.” – Slate
The movie’s interest in accuracy appears to be just about zero. Ann McKee, a CTE researcher who performed much more research into CTE and was far more competent and reliable than Omalu, was removed from the narrative.
McKee would have made a fabulous character in Concussion, by the way, but alas her presence might have made Omalu seem less important. She and her colleagues were snipped out of the narrative, Bechdel test be damned. – Slate
The behavior of those associated with the movie undermines the argument of the article you are reading because it’s unlikely any of the people involved with the film were Nigerian. Yet, they demonstrate a similar disregard for the truth, as did Omalu. This is a ridiculous situation where the initial exaggerations of Omalu were magnified by the movie producers and writers, who desired to create such a simplistic black-and-white narrative (noble Nigerian doctor versus evil NFL organization) that they massively exaggerated the case. One of the producers we recognize is Scott Free Productions, run by the famed director Ridley Scott, who has produced some highly inaccurate historical movies, including the Kingdom of Heaven and 1492: Conquest of Paradise.

Mike Webster has consistently been referred to as the first NFL case of CTE. Most media coverage of Mike Webster has placed his early death at 50 to CTE. Therefore, reading the following history of Mike Webster was shocking.
Maybe that’s the emotional truth, as Landesman would have it: Webster may not have really killed himself, but the head-trauma–induced downward spiral of his life surely amounted to a suicide in slow motion.
The real-world facts are much more complicated, however. Webster was depressed, divorced, a former steroid user, hooked on painkillers and Ritalin. And according to League of Denial, the best and most complete account of football’s concussion crisis, Webster’s risk factors for collapse were legion. A victim of ghastly child abuse with two alcoholic parents, he had mental illness running through both sides of his family. His uncle killed himself. His mother had a nervous breakdown. All four of his siblings were bipolar; one attempted suicide several times; another ended up in prison. – Slate
How is it possible that this background was not widely brought up, and CTE has taken the entirety of the blame for Mike Webster’s early passing?
The following quotation also raises the question of the chicken or egg nature of the relationship between depression and cognitive impairment.
Here’s another just-so story. It’s well-established that depression on its own produces cognitive impairment: Meta-analyses of the research literature suggest that people in the midst of a major depressive episode will flounder on tests of recall and recognition; they’re often unable to concentrate and have other deficits of the sort ascribed to Duerson, Seau, and the others. So perhaps these men grew depressed in the years after their retirement, as some people do.
It is not the author’s conclusion that there is no such thing as CTE. CTE was simply a renaming of a condition studied in boxers as far back as 1928, which was called pugilistic dementia, and was given a broader term as the victims were also football players. The issue is that Omalu appears to have exaggerated and falsified his research to increase massively is reputation and his income. He scammed the US medical system and reduced the reliability of medical research in the area of CTE.
Omalu was not a medical researcher. He performed the autopsy on Mike Webster because he lived in Pittsburg and was a medical examiner when Mike Webster died in 2002. And he has been in arguments with actual researchers who know far more than he does.
In an interview that we watched from Frontline, Omalu showed a bizarre way of coming to conclusions for a medical doctor. He appears to have concluded that Mike Webster must have had brain damage because he played a violent sport (like, as he said, boxers). He stated that he “talked to Mike” when he was examining Webster’s body and asked that Mike help him prove that his life problems were due to CTE. Omalu did not consider any of Mike Webster’s background when concluding that Webster had CTE. In Omalu’s mind, the relationship was that Mike Webster played a violent sport and then had problems in his life after retiring, and therefore his problems were caused by brain trauma.
In the interview, he also states that CTE had no term defined for it at that time, back in 2002, even though the term CTE was coined in the late 1940s. Therefore, he is lying in the interview by stating that he invented how Omalu continues to have credibility after the Frontline interview, which is very odd.
Why would a medical examiner be considered a researcher? In explaining the story, Omalu demonstrates no scientific thinking ability and declares that he talks to the dead because he believes in the afterlife. He continually talks about making promises to the dead people on which he is performing autopsies. He also thinks that God gave Omalu a cross to bear.
He looks like a very amateur doctor who probably received inadequate training in thinking in Nigeria.
We found this interesting quote in the Washington Post article.
I always knew this would eventually be brought to light.
I knew because I have been working with Nigerian people for 30 years.
I know of no other culture with as strong a propensity for hyperbole, overstatement, embellishment and at times, outright lies.
It is in their DNA.
Bennet Omalu is one such example.
And this one..
I think it has a lot to do with their high levels of religiousness. A religious mind thinks that as long as you say something with conviction, go through the motions of showing that you really believe, present your case as if you’re preaching, tell a good story, etc., then other people fall far it. They have learned that that works in religious temples, so they use the same techniques in regular interaction too.
Why would European-based countries want medical doctors from a country where this is a fundamental feature of their culture?
Nigeria is one of the fastest-growing countries in the world in population, yet religious leaders continue to push back on contraception and family planning.
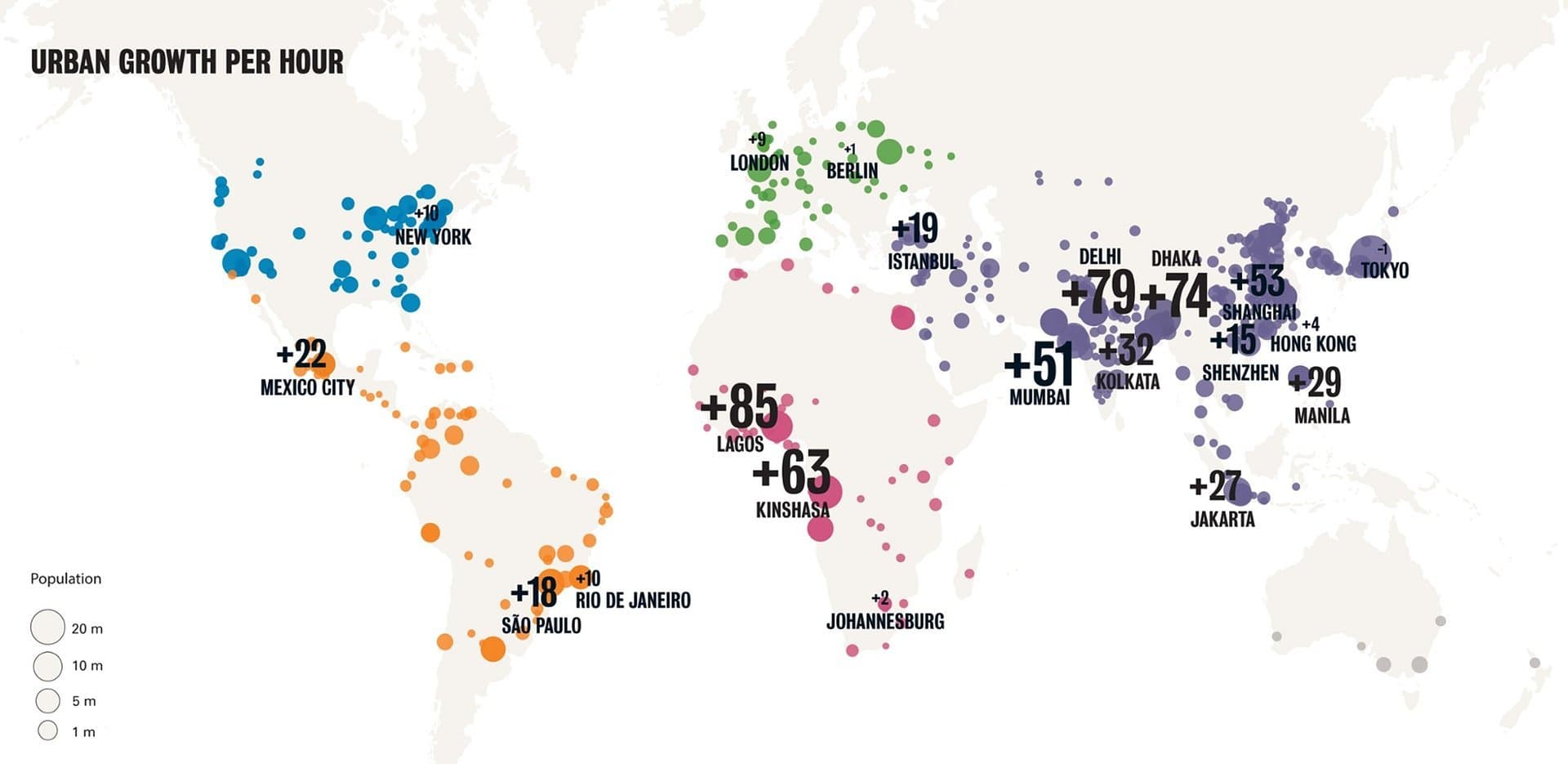
Lagos is the fastest-growing city in the world. Did it occur to the doctors who were quoted earlier in this article that Nigeria could improve its condition by using birth control and that many of the problems driving them from Nigeria are related to uncontrollable population growth? The average Nigerian woman has 5.7 children.
Notice the other fastest-growing cities shown on the graphic, such as Delhi, which is in India — another country aggressively exporting its population to the developed world while doing nearly nothing related to birth control. Dhaka, another massively overgrowing country, is in Bangladesh, which is also being exported, but more to the Middle East’s Gulf region.
Some excellent views are presented here, but this is a better-educated group of Nigerians. Several notable Muslim commenters think that God determines the number of children. The problem is that Nigeria is doing nothing about its out-of-control population growth.
In Africa, albinos have their limbs severed for use in witch doctor rituals. Is this the continent where we want to source doctors from? Is there some problem in educating sufficient numbers of doctors in the first world?
Normally, Africans and Western progressives will bend over backward, blaming any issue in Africa on colonialism. Unfortunately, there is no precedent for using albino limbs in colonial countries, and thus, there is no tie to colonialism. Saddened by this (not the severing of albino limbs, but the inability to blame it on the “legacy of colonialism”), Western progressives move to plan B, ignoring the topic. Hence, they have with the treatment of albinos in Africa.
Albino libs sell for up to $1000 each in Africa.
Conclusion
There has been a strong tendency to accept professionals coming from third world countries into the US. However, in each case where this has occurred, the professional standards in that area have declined. For example, the immigration of large numbers of Indians to the US and Europe has greatly degraded the business practices in IT in both regions due to the fundamental dishonesty of Indians. Indians and Indian firms have been routinely caught defrauding the H1-B program, and virtually no Indian’s professional opinion can be trusted on technical matters as it simply ties back to their financial incentives. The US has greatly declined as a culture since I grew up in the 1980s. A primary reason is the importation of many people from 3rd world nations — the vast majority of whom only care about stealing from the US as quickly as possible. No society can function at a standard white cultural level, with such large numbers of people without a white culture being allowed in the country. The US is now filled with cities or areas that I drive around.
White or European-based societies are not more effective than third-world nations only because they have the technology and because there are “rules of the road” that are followed by people who are native to those societies. Nigeria, India, and similar places do not have the same culture or set of accepted rules as do European-based societies. Even within Africa, Nigerians are known as scammers. Numerous Africans have told me this.
These types of videos are common among Nigerian scammers.
And Omalu is yet another Nigerian scammer, but this time with a degree. Omalu successfully scammed the US medical system because he was not profiled as a Nigerian doctor, who came from a system where running scams is a customarily accepted part of the culture. I would not have had to have been told that Omalu was providing false information. The fact that he was from Nigeria gave me the information I needed. The more Nigerian doctors that arrive in the US and Europe, the more scams we will face.
Declining Professional Standards in White Societies as They Become Infiltrated by Non-Whites
The acceptance of professionals from third-world nations threatens the professional standards and the functioning systems that European-based societies rely upon. They strongly tend to bring corruption from those countries into European-based societies.
![]()
Transparency International ranks Nigeria as the 146th most corrupt country globally, out of roughly 180 countries. That corruption is not just a matter of the government but embedded in the people’s culture. When Nigerian doctors immigrate to white European-based countries (which, according to them, they deserve to leave as living in black-run countries is unacceptable), do they leave their corruption behind them? Where does corruption exist — is it in the country or the people?
The progressive view is that people who immigrate from corrupt countries do not behave corruptly in the countries they immigrate to, which is just bizarre. They move to countries that often do not have natural defenses against such corrupt behavior. For example, in the three decades that Indians have immigrated in large numbers to the US, they have developed a horrible reputation for corruption, often mistreating US citizens, drastically reducing the ethical and work standards in IT, and exploiting other Indians. It should have been obvious this would occur once one observes the standards of behavior and business ethics in India.
People from third-world countries will often complain about their home countries’ dysfunctional nature, using this as an excuse to emigrate to a (nearly always white country). However, if the dysfunctionality is not part of their culture, and indeed part of the culture of the people living in these countries, where does it come from?
The original accusation from these third-world countries is that denying people from third-world countries into white countries is racism, but this question should be asked.
Why do they so desperately need to gain entry into white countries, instead of merely raising their level of their countries?
In the US, we now have a scandal with a US Representative, Ilhan Omar, a refugee from Somalia who married her brother to give him citizenship. She is currently angling for ICE to be abolished and for the US to be borderless essentially. How much should US citizens continue to allow in people who draw down the US’s standards and see the US as an infinite box to pull from? All of the people who live in countries that no one wants to move to want a “borderless” world so they can invade countries they could never have created on their own.
If we are repeatedly told that no culture is superior to any other cultures, why can’t standards be raised easily in these third-world nation countries? Furthermore, why do people from highly corrupt countries have the right to migrate to countries with far lower levels of corruption?
The Response of Some Nigerians to the Article
Several Nigerians have proposed that they do not like this article. Articles like this, they think, could reduce their ability to leave black-run countries. Nigeria, which refuses to use birth control, will grow its population to 800 M by 2100.
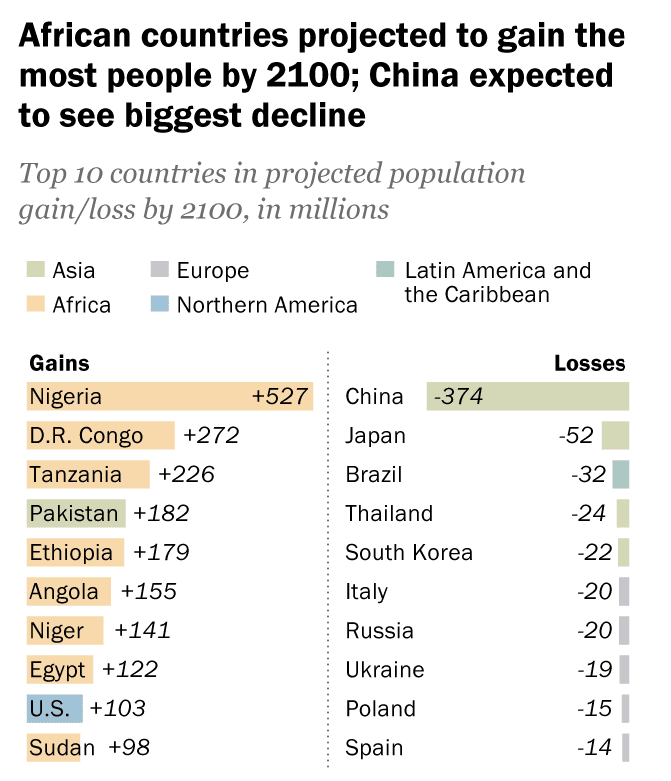
Even though 1/2 of Nigerians live on less than $1 per day, Nigeria has decided that the best course of action is to be the fastest-growing national population in the world.
Nigeria refuses to be recognized — which is perhaps the only thing that can save it, but they need a white savior. Large numbers of Nigerians need white countries to allow them to immigrate. This is why some Nigerians have stated that they do not like this article.
But we don’t change articles for any reason. White countries need to begin forcing African countries to figure out their problems. Secondly, bringing in Nigerian doctors is terrible for the country. Because of their culture, Nigerian doctors are not reliable sources of medical information.
*Commenting Guidelines for Nigerians*
This article receives comments..mostly from Nigerians complaining about the article in broken English.
The first thing for Nigerians to realize is that this article is not written for Nigerians. This article was written for people in European countries to warn them about Nigerians. We do not care what Nigerians think about this article or their views. All comments from Nigerians on this article are deleted upon receipt, and we will not post comments from Nigerians or waste time debating Nigerians in the comments.